The Placenta: A Dynamic Interface of Pregnancy
The placenta is a temporary, fetal-derived organ that supports pregnancy by connecting maternal physiology with fetal development. It is not simply a barrier. It senses changes in the maternal environment and adjusts transport, vascular, endocrine, and immune functions that help regulate fetal growth.
In the Cariaco Lab, we study the placenta as an active biological interface. We ask how maternal signals such as metabolism, inflammation, oxygenation, medications, and environmental exposures reshape placental structure and function. This interface relies on specialized cell layers, such as the syncytiotrophoblast, which is in direct contact with maternal blood, and immune residents like Hofbauer cells that help maintain a healthy environment.
A Temporary Organ with Many Jobs
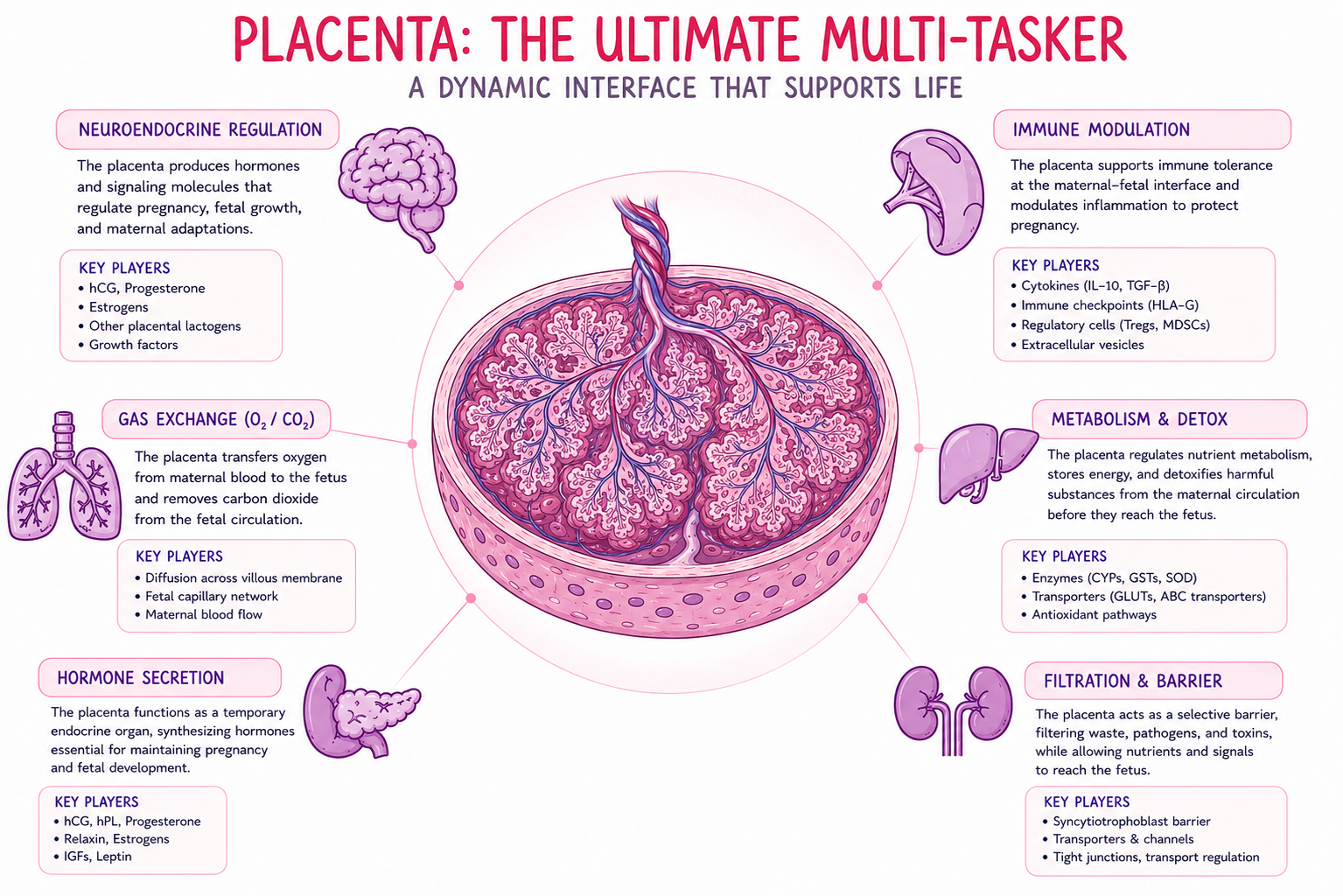
During pregnancy, the placenta supports many functions that fetal organs cannot yet perform on their own. It transfers oxygen and nutrients, removes waste products, produces hormones, regulates immune communication, and helps coordinate maternal–fetal exchange. Figure 1 illustrates the distinct pathways the placenta manages—from neuroendocrine regulation to immune modulation and detoxification—highlighting the specific key players driving each process.
A Sensor of Resilience and Dysfunction
Maternal stressors such as poor nutrition, metabolic imbalance, inflammation, medication exposure, or toxicant exposure can alter placental tissue architecture, immune signaling, transport capacity, and protein expression. These changes may reveal how the placenta responds to stress before clinical symptoms are visible.
In some pregnancies, the placenta compensates and continues to support fetal growth. In others, these adaptive responses are overwhelmed and shift toward dysfunction. Our research aims to identify the molecular and structural features that distinguish resilience from early failure.
The Vascular Tree: Building the Exchange Surface
The placenta contains a dense network of fetal blood vessels organized within tree-like chorionic villi. These villi are surrounded by maternal blood in the intervillous space, bringing maternal and fetal circulation into close proximity while keeping the two blood supplies physically separated.
A successful pregnancy also requires remodeling of maternal spiral arteries. These arteries normally transform from narrow, high-resistance vessels into wider, low-resistance channels that deliver blood to the placenta. When vascular remodeling or villous vascular development is disrupted, oxygen and nutrient exchange can be compromised, contributing to fetal growth restriction and placental dysfunction.
Decoding Human Pregnancy Through Preclinical Models
Many key mechanisms of placental development cannot be tested directly during human pregnancy. Mouse models allow controlled studies of maternal exposures, gene function, placental development, and fetal outcomes. They are especially useful for testing cause-and-effect relationships.
Translation, however, requires careful attention to species-specific anatomy. Mouse and human placentas share important biological principles, including hemochorial organization, trophoblast differentiation, and maternal–fetal exchange. They also differ in tissue architecture, trophoblast invasion, vascular organization, and developmental timing.
The following table summarizes the key developmental and functional differences between human and mouse placentas.
| Feature | Human Placenta | Mouse Placenta |
|---|---|---|
| Overall Shape | Discoid, with a villous exchange structure. | Discoid, with a labyrinthine exchange structure. |
| Main Exchange Region | Tree-like chorionic villi containing fetal vessels surrounded by maternal blood in the intervillous space. | A labyrinth zone where fetal capillaries and maternal blood spaces are closely interdigitated. |
| Trophoblast Invasion | Extravillous trophoblasts invade the decidua and inner myometrium and contribute to spiral artery remodeling. | Trophoblast invasion is more limited and involves species-specific trophoblast populations, including trophoblast giant cells and glycogen trophoblasts. |
| Gestational Timeline | Approximately nine months, allowing prolonged placental growth, branching, and maturation. | Approximately 19–21 days, with rapid placental development that supports a short pregnancy and larger litters. |
| Translational Value | Provides direct relevance to human placental biology and pregnancy complications. | Enables controlled maternal environmental perturbations, genetic manipulation, and mechanistic testing. |
What the Cariaco Lab Studies
The Cariaco Lab combines placental biology, experimental models, human tissue datasets, histology, molecular profiling, and computational image analysis to study how maternal exposures reshape placental structure and function.
To answer these questions, our lab bridges classic placental histology with computational pathology. We design automated digital pipelines alongside molecular profiling approaches to connect tissue architecture, cellular organization, and biological function.
- Costa MA. The endocrine function of human placenta: an overview. Reproductive BioMedicine Online. 2016;32(1):14–43.
- Soncin F, Natale D, Parast MM. Signaling pathways in mouse and human trophoblast differentiation: a comparative review. Cellular and Molecular Life Sciences. 2015;72(7):1291–1302.
- Albrecht ED, Pepe GJ. Regulation of Uterine Spiral Artery Remodeling: a Review. Reproductive Sciences. 2020;27:1932–1942.
- Burton GJ, Jauniaux E. The placenta in fetal growth restriction: What is going wrong? Placenta. 2020;96:10–18.
- Carter AM. Animal models of human placentation — a review. Placenta. 2007;28 Suppl A:S41–S47.
- Rusidzé et al. Comparative placental vascularization and maternal–fetal barrier organization. Cells. 2023;12(4):620.